
EQUITY, EQUITY, EQUITY
As expected, the public portion of the first session of the seventh meeting of the Working Group for amendments to the International Health Regulations (WGIHR) was dominated by calls for equity.


Please watch some excerpts from the first session of the seventh meeting of the WGIHR…

https://rumble.com/v4bhqcb-equity-equity-equity.html
Click on the link below to watch the entire public session…
The remaining sessions this week will be conducted in secret. The final session on Friday, February 9, 2024 is scheduled to be live streamed, recorded and made public.

SUMMARY:
MALAYSIA, speaking for the Group for Equity, reiterated their demand that equity be the focus of the negotiations. They want the WGIHR Bureau to focus on Articles 13, 13A, 44, 44A and Annexes 1 and 10.
“Presently, the current proposed texts have been inadequate.”
ESWATINI, speaking for the group of 47 African nations and Egypt, also reiterated their demand that equity be the focus of the negotiations. They want the bureau to focus on Articles 13, 13A, 44, and 44A.
“We therefore wish to express our great concern regarding the slow progress made in discussing equity related proposals.”
BANGLADESH, aligned itself with the statements made by MALAYSIA and ESWATINI, and they also reiterated their demand that equity be the focus of the negotiations.
“It is a fact that in many cases equity related proposals have fallen apart despite the strong demand of a large number of countries.”
ZAMBIA also reiterated their demand that equity be the focus of the negotiations.
“For Zambia, the need for equity as a guiding principle of the revised IHR cannot be over-emphasized.”
JAPAN dropped a bomb (sorry for the irony) during the meeting by REQUESTING THAT THE CURRENT VERSION OF THE PROPOSED TEXT BE MADE PUBLIC.
“Japan is proposing to the bureau and the WGIHR to consider the publication of the Bureau’s text.”
RUSSIA also dropped a couple of bombs during the meeting by revealing that they had received a letter from the Director-General stating that 4 nations had voiced reservations/rejected the 2022 amendments (Iran, New Zealand?, Netherlands? and an unknown fourth nation). Russia also pointed out that this had caused a split in the World Health Assembly and noted that a similar split might result if consensus is not reached in the current negotiations.
“We’d like to point out the Director-General’s letter that four countries have NOT joined amendments adopted two years ago at the WHA. We respect every country’s position. The point is, for one single amendment, for one amendment alone, four countries have made reservations. To avoid such a situation on a whole series of amendments we are addressing now, maybe we have to think about stages for a final agreement. How can we avoid having this stand-off situation for a whole range of amendments?
The THIRD WORLD NETWORK basically accused the WGIHR bureau of failing to uphold their promise to hold informal sessions regarding equity, and pointed out that the mandate of the negotiations was to ensure equity. They also called for the Bureau to publish the latest version of the text proposals that have been circulating in secret.
“We request the Bureau to kindly publish the text proposals to the member states in the interest of transparency.”
We stand here until now with not a single provision which creates a legal obligation to serve equity in access to health products.”
“This is the reason why we need Africa Group and Bangladesh proposals on Article 13A and 44A.”
“Most probably the IHR will have a separate set of parties.”
More from the Third World Network
“The Bureau’s proposal for Article 4 perpetuates the inherent inequity of international health emergency law, where communication and coordination are obligatory only for sharing of information about potential public health events.”
“There is not even a guarantee that a State Party’s request for assistance in responding to a disease outbreak will be responded to by WHO or by other States Parties.”
“In addition, the Bureau’s proposal to retain the original text of Article 5 also avoids the proposal to incorporate the differential treatment of the obligation of developing countries in establishing surveillance capacities. Countries like Malaysia have proposed changes to Article 5 to this effect and it has support from a larger number of developing countries, but the text is not reflected in the Bureau’s proposal for Article 5 in any manner whatsoever.”
CLICK HERE for a detailed view on what is REALLY going on at these negotiations.
The INTERNATIONAL FEDERATION OF PHARMACEUTICAL MANUFACTURERS AND ASSOCIATIONS presented the Big Pharma hypocritical position by rejecting the calls for access to their “intellectual property” while demanding data sharing in regards to pathogens and genomic sequences from the nations. Transparency from thee, but not from me!
“We must preserve what worked well and ensure rapid access to public health data in pandemic situations.”
“Improving IHR is imperative for ensuring the timely exchange of public health data, including pathogen and epidemiological data.”
OXFAM hit a grand slam in demanding equity, calling for an end to Big Pharma’s monopoly, the removal of intellectual property barriers and an end to the world’s double standard by calling for health to take precedence over commercial interests.
“We urge you to quickly adopt concrete measures to ensure timely, equitable access to medical technologies in order to protect all populations.”
“Business as usual of monopoly on medical technology clearly failed.”
“The definition of insanity is doing the same thing and expecting different outcomes.”
“This means that all member states prioritize public health for all people over commercial interests. Therefore, all member states should commit to fair allocation of medical products relevant to health crisis according to health needs, not ability to pay.”
“Enabling local production in the Global South through commitment to sharing knowledge and technology, removing IP barriers and investing in manufacturing.”
“Implementing conditionality on public funding for R&D and on purchasing agreements that mandate sharing technology and know-how with researchers, developers and producers in the Global South and removing IP barriers.”
“Sharing pathogens must be combined with sharing the benefits resulting from sharing the pathogens, otherwise it’s illogical and immoral.”
“To protect their people from COVID, and potential pandemics, countries in the Global North implemented and proposed policies that they object to here. They must stop the double standard and instead, make concessions to ensure that all populations are protected irrespective of where they live.”
SOUTH CENTER reiterated the call for equity to be addressed in both negotiations.
“It is critical that these proposals on equity, in particular Articles 13, 13A, 44 and 44A are prioritized and treated on an equal footing with other amendment proposals.”

The disagreements center around the proposed amendments to Articles 13, 13A, 44, 44A and Annexes 1 and 10.
The pertinent documents are here…
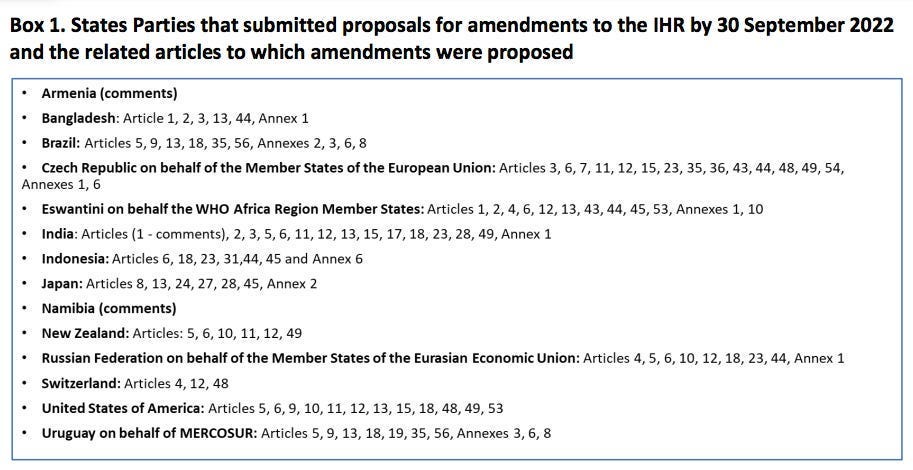
Originally submitted proposed amendments revealing the nations that submitted them:
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_6-en.pdf
or…
https://apps.who.int/gb/wgihr/pdf_files/wgihr1/WGIHR_Submissions-en.pdf
Summary of the amendments that do not specify which nation proposed which amendment:
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_7-en.pdf
The Final Report of the International Health Regulations Review Committee:
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_5-en.pdf

THE AFRICA GROUP
New Article 13A
Access to Health Products, Technologies and Know-How for Public Health Response
1. Immediately after the determination of a public health emergency of international concern under Article 12, the Director General shall make an immediate assessment of availability and affordability of required health products and make recommendations, including an allocation mechanism, to avoid any potential shortages of health products and technologies pursuant to Article 15 or 16 as appropriate.
2. States Parties shall co-operate with each other and WHO to comply with such recommendations pursuant to paragraph 1 and shall take measures to ensure timely availability and affordability of required health products such as diagnostics, therapeutics, vaccines, and other medical devices required for the effective response to a public health emergency of international concern.
3. States Parties shall provide, in their intellectual property laws and related laws and regulations, exemptions and limitations to the exclusive rights of intellectual property holders to facilitate the manufacture, export and import of the required health products, including their materials and components.
4. States Parties shall use or assign to potential manufacturers, especially from developing countries, on a non-exclusive basis, the rights over health product(s) or technology(ies), when the same is/are obtained in the course of research wholly or partially funded by public sources, and is/are identified as required health product(s) or technology(ies) to respond to a PHEIC, with a view to ensure equitable, timely availability and affordability through diversification of production.
5. Upon request of a State Party, other States Parties or WHO shall rapidly cooperate and share relevant regulatory dossiers submitted by manufacturers concerning safety and efficacy, and manufacturing and quality control processes, within 30 days. The dossiers received by a requesting State Party shall be solely used by their regulatory authorities and manufacturers designated by the requesting State Party for the purposes of accelerating the manufacture and supply of product(s) or technology(ies) as well as expediting their regulatory approval. Requesting State Party shall take measures to prevent designated manufacturer(s) from disclosing such information to a third-party(ies) except for the purposes of producing and supplying any materials or components to the manufacturer(s) under a contract with non-disclosure provisions.
6. WHO shall take measures to ensure availability and accessibility through the local production of required health products including: (
a) develop and publish a list of required health products,
(b) develop and publish specifications for the production of required health products,
(c) develop appropriate regulatory guidelines for the rapid approval of health products of quality including development of immunogenicity co-relative protection (ICP) for vaccines,
(d) establish a database of raw materials and their potential suppliers,
(e) establish a repository for cell-lines to accelerate the production and regulatory of similar biotherapeutics products and vaccines,
(f) review and regularly update WHO Listed Authorities so as to facilitate appropriate regulatory approvals,
(g) any other measures required for the purposes of this provision.
7. The States Parties shall take measures to ensure that the activities of non-state actors, especially the manufacturers and those claiming associated intellectual property rights, do not conflict with the right to the highest attainable standard of health and these Regulations and are in compliance with measures taken by the WHO and the States Parties under this provision, which includes:
(a) to comply with WHO recommended measures including allocation mechanism made pursuant to paragraph 1.
(b) to donate a certain percentage of their production at the request of WHO.
(c) to publish the pricing policy transparently. (d) to share the technologies, know-how for the diversification of production.
(e) to deposit cell-lines or share other details required by WHO repositories or database established pursuant to paragraph 5.
(f) to submit regulatory dossiers concerning safety and efficacy, and manufacturing and quality control processes, when called for by the States Parties or WHO.
BANGLADESH
NEW Article 13A
WHO Led International Public Health Response
1. States Parties recognize WHO as the guidance and coordinating authority of international public health response during public health Emergency of International Concern and undertake to follow WHO’s recommendations in their international public health response.
2. WHO shall carry out an assessment of the availability and affordability of the heath products such as diagnostics, therapeutics, vaccines, personal and protective equipment and other tools required for responding to public health emergencies of international concern, including the potential increase in supply resulting form the surge and diversification of production and in cases of expected shortage of supply, WHO shall develop and allocation plan for health products so as to ensure equitable access to people of all States Parties.
3. WHO shall, in its allocation plan for health products, inter alia identify and prioritize the recipients of health products, including health workers, frontline workers and vulnerable populations, and determine the required quantity of health care products for effective distribution to the recipients across States Parties.
4. Upon request of WHO, States Parties with the production capacities shall undertake measures to scale up production of health products, including through diversification of production, technology transfer and capacity building especially in the developing countries.
5. Upon request of WHO, States Parties shall ensure the manufacturers within their territory supply the requested quantity of the health products to WHO or other States Parties as directed by WHO in a timely manner in order to ensure effective implementation of the allocation plan.
6. WHO shall develop and maintain a database containing details of the ingredients, components, design, know-how, manufacturing process, or any other information required to facilitate manufacturing of health products required for responding to the potential public health emergencies of international concern. Within two years of the entry into force of this provision, WHO shall develop this database for all PHEICs declared so far, including for the diseases identified in the IHR 1969.
7. In accordance with the provisions of these Regulations and in particular Article 13A (1), shall collaborate with other international organizations, and other stakeholders consistent with the provisions of FENSA, for responding to public health emergency of international concern. WHO shall report all its engagement with other stakeholders to the Health Assembly. The Director-general shall provide documents and information relating to such engagements upon request of States Parties.
THE AFRICA GROUP
New Article 44A
Financial Mechanism for Equity in Health Emergency Preparedness and Response
1. A mechanism shall be established for providing the financial resources on a grant or concessional basis to developing countries. Such financial mechanism shall provide the financial assistance to achieve the following purposes:
(i) building, developing, strengthening, and maintaining of core capacities mentioned in Annex 1;
(ii) strengthening of Health Systems including its functioning capacities and resilience;
(iii) building, developing and maintaining research, development, adaptation, production and distribution capacities for health care products and technologies, in the local or regional levels as appropriate.
(iv) addressing the health inequities existing both within and between States Parties such that health emergency preparedness and response is not compromised;
2. The WHA shall make arrangements to implement the above-mentioned provisions, within 24 months of the adoption of this provision, reviewing and taking into existing availability of funds and WHO arrangements for health emergency preparedness and response and whether they shall be maintained. Every four years thereafter, the WHA shall review the financial mechanism and take appropriate measures to improve the functioning of the mechanism. WHA shall also ensure that the financial mechanism functions under the guidance of and be accountable to States Parties, which shall decide on its policies, programme priorities and eligibility criteria.

I originally addressed these issues more than a year ago.
THE ELEPHANT IS STILL IN THE ROOM!
Please read the articles below…

Let's Talk About The Elephant In The Room

NOTE: So as to not influence the reader, this article is published without any of my opinions, except this: Something seems very, very, very wrong here! Please take the time to really review this information thoroughly before commenting. I look forward to reading your INFORMED opinions.

Corporate Colonialism

CLICK HERE to #EnforceArticle55 Today (February 1, 2024) is the one year anniversary of the publication of the WHO’s “Zero Draft.” Please watch the videos below…

The World Health Assembly is Exceeding its Authority

I submitted the following information as my public comment to the Office of Global Affairs in regards to the proposed amendments to the International Health Regulations.

The WGIHR missed their deadline and are attempting to violate Article 55 of the International Health Regulations.


LEARN MORE:
ThePeoplesDeclaration.com
ExitTheWHO.org
ExitTheWHO.com
StopTheGlobalAgenda.com
StopTheAmendments.com
StopTheWHO.com
ScrewTheWHO.com
MaskCharade.com
RejectDigitalEnslavement.com
HealthFreedomBillOfRights.com
PreventGenocide2030.org
DoorToFreedom.org

James Roguski
The old system is crumbling, and we must build its replacement quickly.
If you are fed up with the government, hospital, medical, pharmaceutical, media, industrial complex and would like to help build a holistic alternative to the WHO, then feel free to contact me directly anytime.
JamesRoguski.substack.com/about
JamesRoguski.substack.com/archive
310-619-3055
All content is free to all readers.
All support is deeply appreciated.
From what I hear no one cares what the people think. They are ready too jam these amendments one way or another. It's obvious that all these countries don't care about there people but the revenue that will come with these negotiations. These heathens care only about the equity,power, enslavement. The outside influence too stop this seems in vain. The WHO will disregard any outside influence. I wonder what else can be done. Mr James Roguski just wanted too say you've been a hell of a warrior in this battle. I pray God will intervene in this urgent matter
Just when I thought I had reached maximum dislike of the word “equity” I find there’s room for more aversion . . .
Appreciate so much your perseverance in following and reporting on this ongoing global travesty.