
The Final Report of the International Health Regulations Review Committee
The International Health Regulations Review Committee (IHRRC) published their final report and they have validated nearly everything that I have been saying for the last month and a half. Go figure.


For well over a month, I have been stating my concerns regarding the following aspects of the proposed amendments to the International Health Regulations:

Today, the International Health Regulations Review Committee (IHRRC) published their Final Report
Final Report of the International Health Regulations Review Committee regarding the proposed amendments to the International Health Regulations
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_5-en.pdf
I must admit. I am pleasantly SURPRISED.
Is it possible that my prayers have been answered?
Below are the TOP 10 things that I have been speaking up against followed by excerpts from the IHRRC Report.
For the most part, it seems like the IHRRC agrees with me.
Go figure.

In their final report, the IHRRC stated:
Article 1- Definitions
In relation to the two proposed amendments to remove the word “non-binding” from the definitions of “temporary” and “standing recommendations”, the Committee notes that on a plain reading the proposed change would not affect the current understanding of the definition of standing or temporary recommendations as merely advice that is not mandatory. However, given that substantial proposals were made in relation to WHO recommendations in other related articles, the proposed amendments to these definitions could be understood as aiming to change the nature of these recommendations from non-binding to binding, and giving a binding effect to WHO recommendations and requests as proposed in other articles. That change would require a fundamental reconsideration of the nature of recommendations and the process for their adoption and implementation. The Committee further notes that during a public health emergency of international concern the recommendations may work better if they are not mandatory and advises against changing the nature of recommendations.
-Page 26
Article 42 – Implementation of health measures
The proposed amendments expand the scope of Article 42 in three ways: by making specific reference to recommendations made under Articles 15 and 16 (temporary and standing recommendations);
The proposed amendment to include a reference to temporary and standing recommendations seems to make application of these recommendations obligatory.
-Page 67

In their final report, the IHRRC stated:
Article 2 – Purpose and scope
The Committee considers that the proposed amendment to replace “public health risk” with “all risks with a potential to impact public health” may not increase the clarity of this Article. Public health risks are already defined in Article 1.
-Page 27

In their final report, the IHRRC stated:
Article 3 – Principles
The Committee strongly recommends the retention of the existing text "full respect for the dignity, human rights and fundamental freedoms of persons” as an overarching principle in the first paragraph, and notes that the concepts of human rights, dignity and fundamental freedoms are clearly defined within the framework of treaties to which many of the States Parties to the Regulations have adhered. The inclusion of human rights in Article 3 of the current International Health Regulations (2005) was a major improvement on the previous 1969 Regulations.1 The reference to “respect for dignity, human rights and freedoms of persons” works not only as an overarching principle in Article 3, but also as a concrete reference point in the operationalization of all articles concerning public health response, response measures, additional health measures and recommendations.
-Page 28

In their final report, the IHRRC stated:
NEW Article 13A – Access to health products, technologies and know-how for public health response
This proposed new Article addresses a range of considerations pertaining to the availability and affordability of health products, technologies and know-how. It goes further than the other proposed new Article 13A WHO-led international public health response in that it imposes obligations on States Parties as well as on WHO and it introduces a more robust final paragraph concerning the role and regulation of non-State actors.
WHO recommendations, as currently stated under Articles 15 and 16, were not envisioned for the purposes of establishing a medicines allocation mechanism or otherwise directing States Parties on increasing access to health products.
-Page 52
NEW Article 13A – Access to health products, technologies and know-how for public health response
However, the requirement in paragraph 1 for the Director-General to make an “immediate assessment of availability and affordability of required health products” may not be feasible due to the magnitude of such a list implied by the proposed amendment and the very high workload imposed on WHO during the initial stages of determining a PHEIC .
The Committee has concerns regarding the proposal in paragraph 1 to use Article 15 (temporary recommendations) for the purposes of establishing an “allocation mechanism.” Temporary recommendations, as defined under Article 1, are “non-binding advice and do not authorize WHO to direct States.
A different mode of authority may be required to establish an allocation mechanism.
It is unclear to the Committee what it means to comply with non-binding recommendations as per Articles 15 or 16.
-Page 53
NEW Article 13A – WHO-led international public health response
The Article goes further, however, in attributing to WHO several obligations that it does not currently have under the International Health Regulations (2005), including: to conduct an assessment of availability and affordability of “health products”; to develop an allocation and prioritization plan in the event that such an assessment reveals shortages in supply; and to direct States Parties to increase and diversify production and distributive functions for health products within individual States.
The Article further mandates WHO to establish a database “containing details of the ingredients, design, know-how, and manufacturing process or any other information required to facilitate manufacturing of health products” required to respond to potential PHEICs, and to maintain the database for all past PHEICs, as well as diseases identified in the International Health Regulations (1969).
This proposal also renders mandatory the temporary and standing recommendations addressed under Articles 15 and 16. The State Party making this proposal has also provided corresponding proposals to change the definitions of temporary and standing recommendations under Article 1 to render them coherent with new proposals in paragraph 1 of this proposal for a new Article 13A.
More fundamentally, it remains unclear how WHO could discharge the unprecedented set of new responsibilities attributed to it relating to health products and know-how under this proposed amendment, as these may arguably exceed its constitutional mandate. In order to be legally feasible, this amendment will require coherence with States Parties’ relevant national laws and other international obligations.
-Pages 54-55
NEW Article 13A – WHO-led international public health response
Finally, it is unclear whether reference to “WHO’s recommendations” in this paragraph refers to WHO’s authority to issue non-binding recommendations under Articles 15 and 16, or whether other forms of recommendations are envisioned. If indeed recommendations under Articles 15 and 16 are the targets of this addition in paragraph 1, the addition would be incoherent with the existing Regulations, as it would render these recommendations mandatory, whereas they were intended to be non-binding.
The Committee notes that the same State Party that proposed this new Article, has also put forward amendments to the definitions of temporary and standing recommendations, which propose removing the reference to “non-binding” in these definitions. If read in conjunction with this newly proposed Article, the proposed amendments to remove “non-binding” could be seen as a desire to make the temporary and standing recommendations binding, and therefore legally coherent with Article 13A, paragraph 1.
Similar to this proposal, paragraph 1 in the other proposal for a new Article 13A also makes explicit reference to Articles 15 and 16, and paragraph 2 creates a mandatory obligation on States to cooperate according to Articles 15 and 16.
Irrespective of legal coherence, changing temporary and standing recommendations into binding obligations may raise questions of feasibility. At this moment it is still unclear how to assess “compliance” with temporary recommendations issued during PHEICs, since they are defined as non- binding advice.
-Page 56

The IHRRC did not specifically address the types of “recommendations” that are listed in Article 18 (see below), they did raise concerns regarding articles 1, 13A and 42 that directly relate to the concept of changing non-binding “recommendations” to obligations.
Article 18 Recommendations with respect to persons, baggage, cargo, containers, conveyances, goods and postal parcels
1. Recommendations issued by WHO to States Parties with respect to persons may include the following advice:
– no specific health measures are advised;
– review travel history in affected areas;
– review proof of medical examination and any laboratory analysis;
– require medical examinations;
– review proof of vaccination or other prophylaxis;
– require vaccination or other prophylaxis;
– place suspect persons under public health observation;
– implement quarantine or other health measures for suspect persons;
– implement isolation and treatment where necessary of affected persons;
– implement tracing of contacts of suspect or affected persons;
– refuse entry of suspect and affected persons;
– refuse entry of unaffected persons to affected areas; and
– implement exit screening and/or restrictions on persons from affected areas.

In their final report, the IHRRC stated:
Article 18 - Recommendations with respect to persons, baggage, cargo, containers, conveyances, goods and postal parcels
The first part of the proposal about passenger information is not clear. If the proposed mechanism only concerns affected persons as per Article 1, then the mechanisms described in Articles 30, 37 and 38 and Annexes 8 and 9 can be used. If it is to cover all passengers, this would be a challenge to feasibility.
-Page 60
Article 23 - Health measures on arrival and departure
Regarding the proposal to introduce the possibility for health documents to include information related to laboratory tests, the Committee notes that this was a practice during the COVID-19 pandemic, within the context of the PHEIC and the related temporary recommendations. However, given that Article 23 applies to all situations, not only PHEICs, the Committee is concerned that such a requirement may overburden travellers, and may even raise ethical and discrimination-related concerns.
Lastly, the Committee recommends examining these proposed amendments in conjunction with Articles 31, 32, 35 and 36 and Annexes 6 and 7, as well as with the related proposed amendments thereto. Should any of these amendments be retained, definitions should be provided in Article 1 for the terms “information”, “digital” and “report”.
-Page 62
Article 27 - Affected Conveyances
The Committee considers the proposed amendment to be redundant.
The Committee notes that States Parties’ ability to regulate is subject to the international law of jurisdiction. Depending on the location of conveyance, State Parties may or may not have the legal power to fulfill their newly proposed obligation.
-Page 63
Article 35 - General rule
This Article states that, as a general rule, no health documents, other than those provided for under the Regulations or in recommendations issued by WHO, shall be required in international traffic.
-Page 65
Introducing an obligation for States Parties to recognize the health documents of other States Parties may pose many practical difficulties, especially considering that domestic legislation concerning privacy and personal information protection differs from one State Party to the next. Another concern, depending on how the amendments are implemented, is the appropriate level of protection of personal data under the applicable regional and international instruments.
As a general observation, the Committee recommends that the multiple proposals for amendments related to the digitalization of health information should be addressed in one single article and be harmonized with the provisions of Annexes 6 and 7.
-Page 66
Article 36 – Certificates of vaccination or other prophylaxis
It is unclear how the specifications and requirements for such “other types of proofs and certificates” would be formulated and by whom, since the proposal only mentions a possibility for the Health Assembly to design and approve such certificates. It is also unclear whether “substitutes for” and “complementary to” are to be used interchangeably. This matters because the meaning is different. The proposal that such certificates may include test certificates and recovery certificates should be read in conjunction with the proposed amendments to Article 23, paragraph 1(a), introducing laboratory tests and/or information on vaccination as part of the information that may be required of travellers.
-Page 67
Annex 6
The comments made under Article 35 apply in general to Annex 6, for example, with regard to the feasibility of digital certificates in many countries, as well as not precluding future technological developments. Similar considerations apply to the feasibility of having the Health Assembly decide on the related technical requirements, since situations may change periodically at short notice.
-Page 87
Annex 8
It is unclear to the Committee how this additional question on the maritime declaration will facilitate application of the Regulations.
The issue of the digital format of vaccination cards is being addressed in other proposed amendments to Articles 31, 35 and 36 (see related comments).
-Page 88

In their final report, the IHRRC stated:
Article 43 – Additional health measures
The proposals in paragraphs 4 and 6 establish a quasi-judicial process with tight deadlines and binding effects for recommendations, with the Emergency Committee having the final authority to decide on the appropriateness of health measures. This Committee is concerned that these proposals may unduly impinge on the sovereignty of States Parties and give binding effects to what are supposed to be recommendations.
-Page 68

In their final report, the IHRRC stated:
New Article 44A – Financial mechanism for equity in health emergency preparedness and response
The Committee notes a divergence of views as to whether WHO has a financing function.
The Committee notes that, under Article 44, WHO already has a role, in collaboration with States Parties, to mobilize financial resources, and cautions against creating an explicit financing function for WHO under the Regulations.
-Page 71

The IHRRC did not specifically address the proposed amendment regarding increased censorship powers for the WHO in Annex 1, but they did state the following:
A balance is needed between ensuring more accurate scientific information on one hand and freedom of speech and the press on the other. How to strike that balance while navigating global policy and national regulatory landscapes will be an ongoing challenge.
-Page 21

In their final report, the IHRRC stated:
NEW Annex 10
The obligations set out in paragraph 1 of this proposed new Annex appear to be absolute and unconditional.
If requested to provide assistance, it is unclear what steps WHO or States Parties should take.
In summary, the Committee supports the idea of full cooperation and collaboration between WHO and States Parties, but the proposed new Annex 10 would be difficult to implement.
However, the proposed new Annex 10 goes well beyond that supporting function, containing provisions that exceed the scope of both the current Article 44 and the amendments proposed thereto.
-Page 89

OFFICIAL WHO DOCUMENTS:
https://apps.who.int/gb/wgihr/e/e_wgihr-2.html
1. Provisional Agenda
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_1-en.pdf
2. Draft Program of Work
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_2-en.pdf
3. Proposed Modalities of Engagement For Relevant Stakeholders
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_3-en.pdf
4. Provisional WGIHR timeline 2022–2024
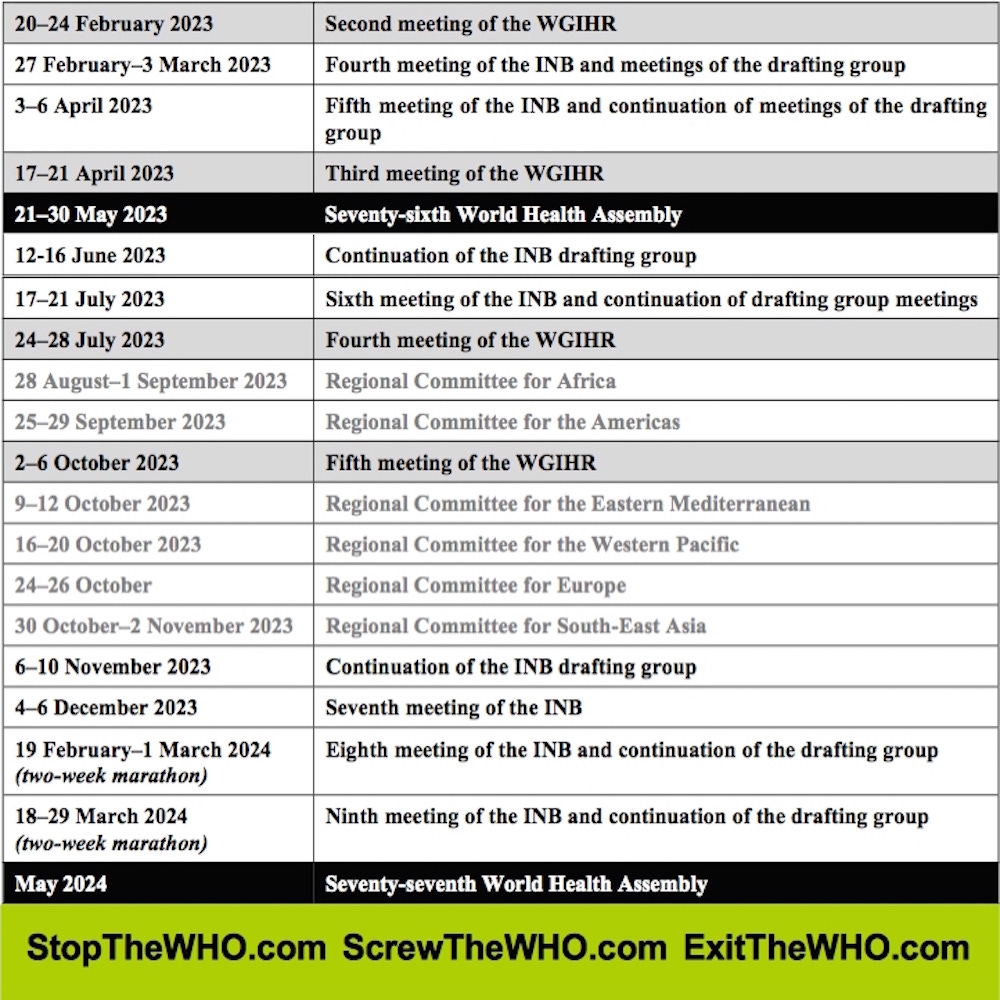
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_4-en.pdf
5. Report of the Review Committee regarding amendments to the International Health Regulations
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_5-en.pdf
6. Proposed amendments to the International Health Regulations
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_6-en.pdf
7. Article-by-Article compilation of proposed amendments to the International Health Regulations
https://apps.who.int/gb/wgihr/pdf_files/wgihr2/A_WGIHR2_7-en.pdf
Report of the Sixth Meeting of the Review Committee regarding amendments to the International Health Regulations (2005) (IHR)

LEARN MORE:
StopTheWHO.com
ScrewTheWHO.com
ExitTheWHO.com

by James Roguski
The old system is crumbling, and we must build its replacement quickly.
If you are fed up with the government, hospital, medical, pharmaceutical, media, industrial complex and would like to help build a holistic alternative to the WHO, then feel free to contact me directly anytime.
JamesRoguski.substack.com/about
JamesRoguski.substack.com/archive
310-619-3055
All content is free to all readers.
All support is deeply appreciated.
Participate in my twice daily ZOOM meetings...
https://jamesroguski.substack.com/p/daily-zoom-meetings
My head is reeling! I have to go and lie down even though I just got up. Does this mean there are actually some humans in the IHRRC? Maybe they have realised they too have to live on this planet. Maybe Africa did stand firm. But we must not let down our guard. We have seen this strategy all too often in the environmental sector. Example: A developer comes along with a proposal that is so outrageous it makes opponents feel physically sick. Say they propose to build 1000 houses in a sensitive wetland. So in the end, after a huge battle, when they come with something somewhat better, say 200 houses, everyone is just too relieved and exhausted and accepts it. When "no development " should have been the only option on the table in the first place. It's a strategy.
Anyway, hopefully this is not the case here. James, how binding is this report on Tedros et al?