This article is a discussion of a hypothesis that MAY explain a number of previously unexplained phenomena.
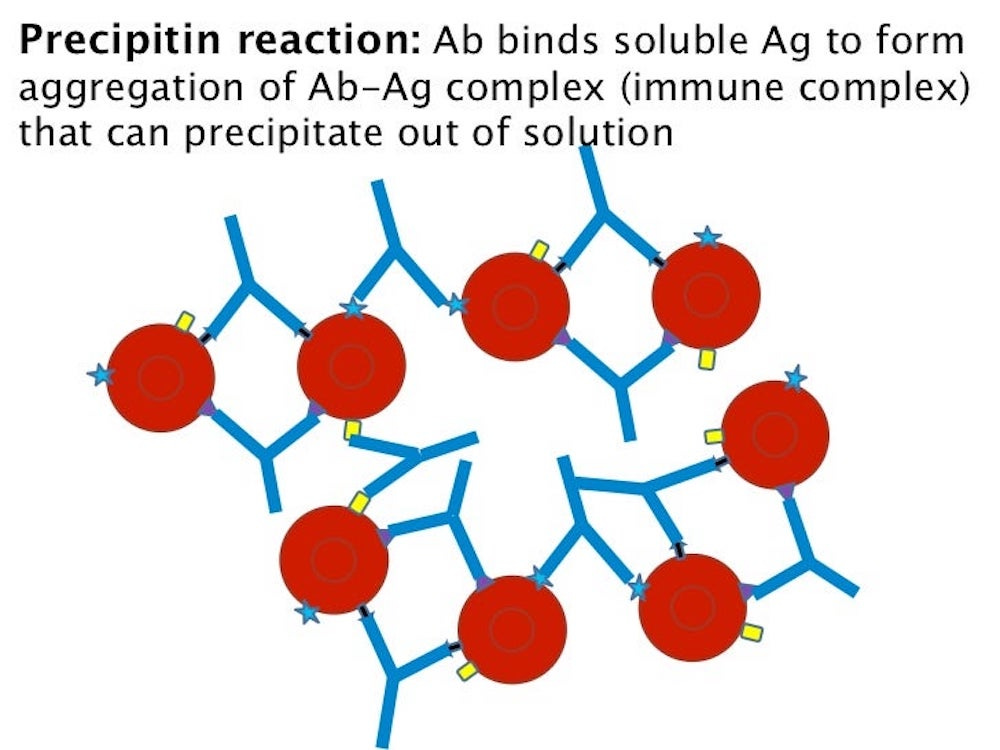
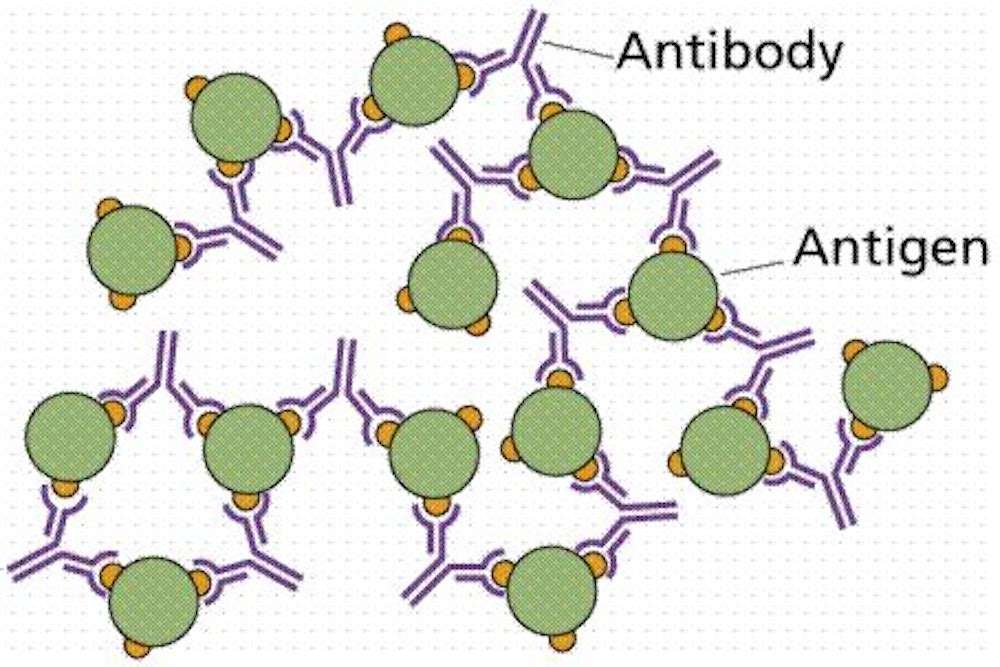
It is a fundamental principle of immunology that when antibodies (Ab) are in the presence of antigens (Ag), the antibody-antigen complex can form cross-links and become large enough to precipitate out of solution.
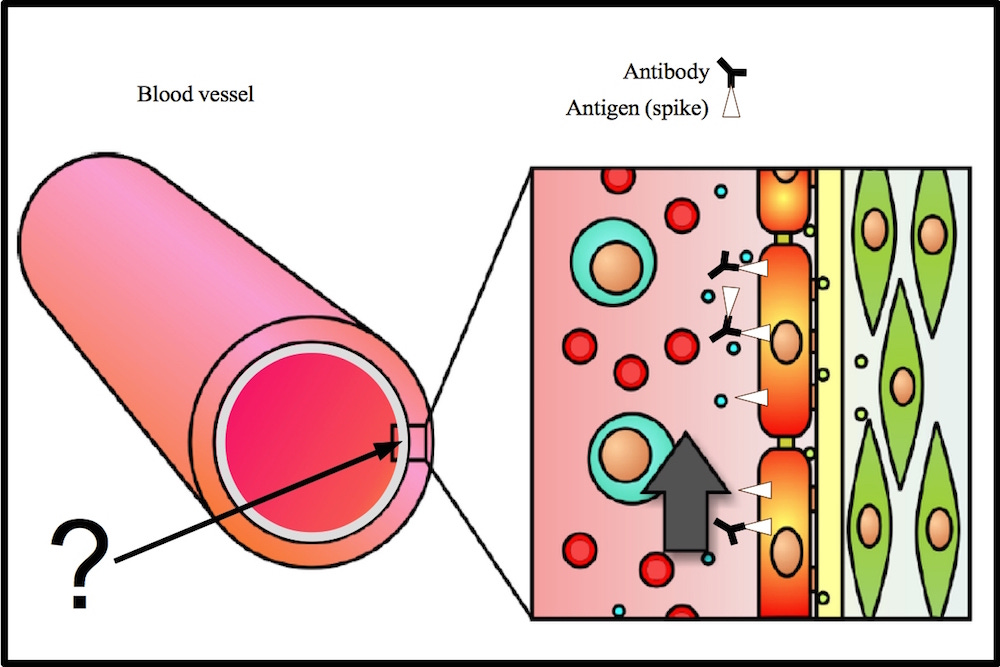
Is it possible that immune complexes (spike protein + antibodies) can form on the lining of arteries? Is it likely? Is it almost a certainty?
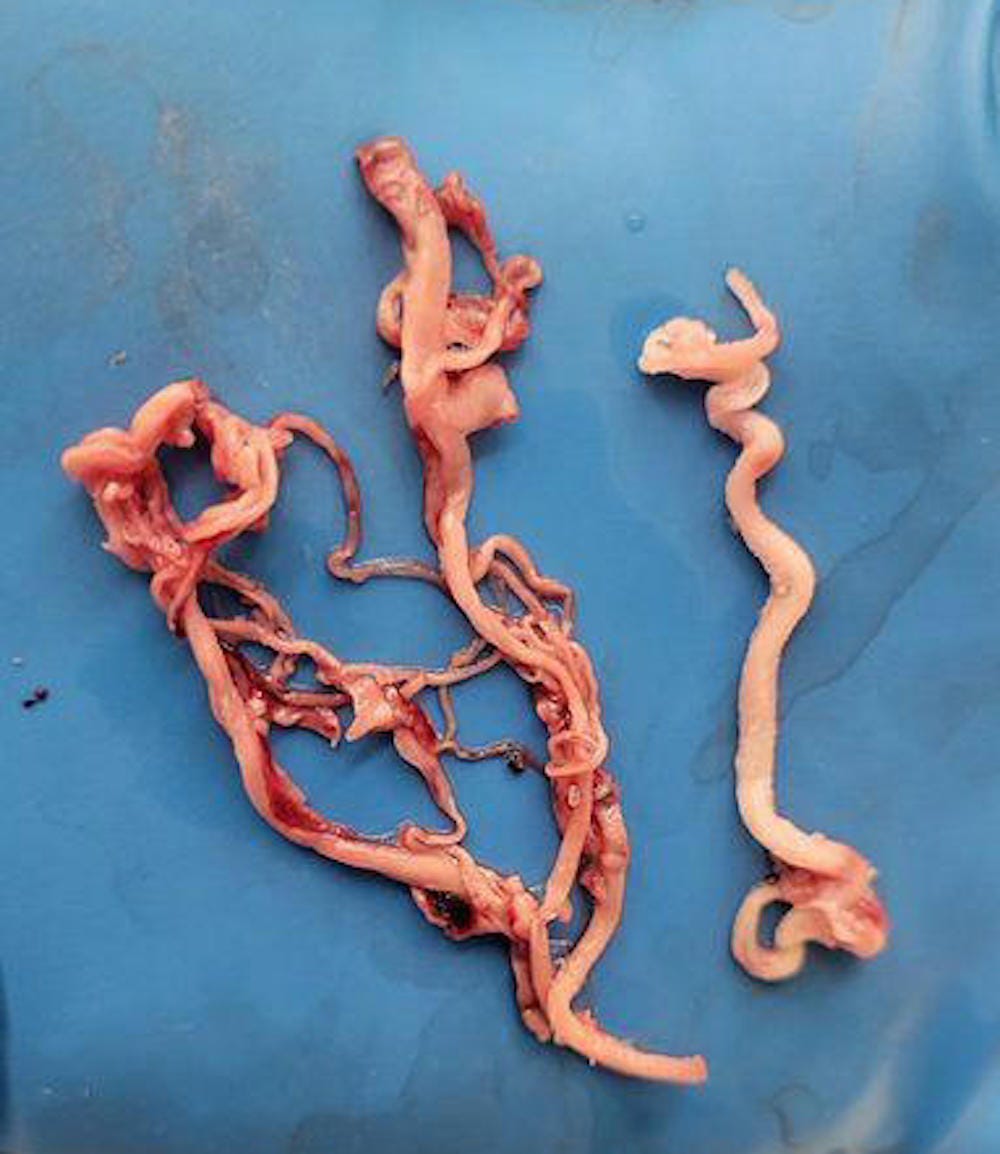
Is it possible that these immune complexes can trigger a cascade of events involving platelets, fibrin (and possibly amyloid protein) that results in the creation of the white, elastic structures that embalmers have been finding in 20-30% of the bodies of the deceased ever since the COVID-19 jabs started to be administered?
Is it possible that smaller “precipitins” can form throughout the body and cause a multitude of diseases?
The scientific method demands scrutiny and discussion of this phenomena and the hypothesis that may explain it.
Post your ideas, opinions, constructive criticisms and/or supportive evidence in the comment section below…
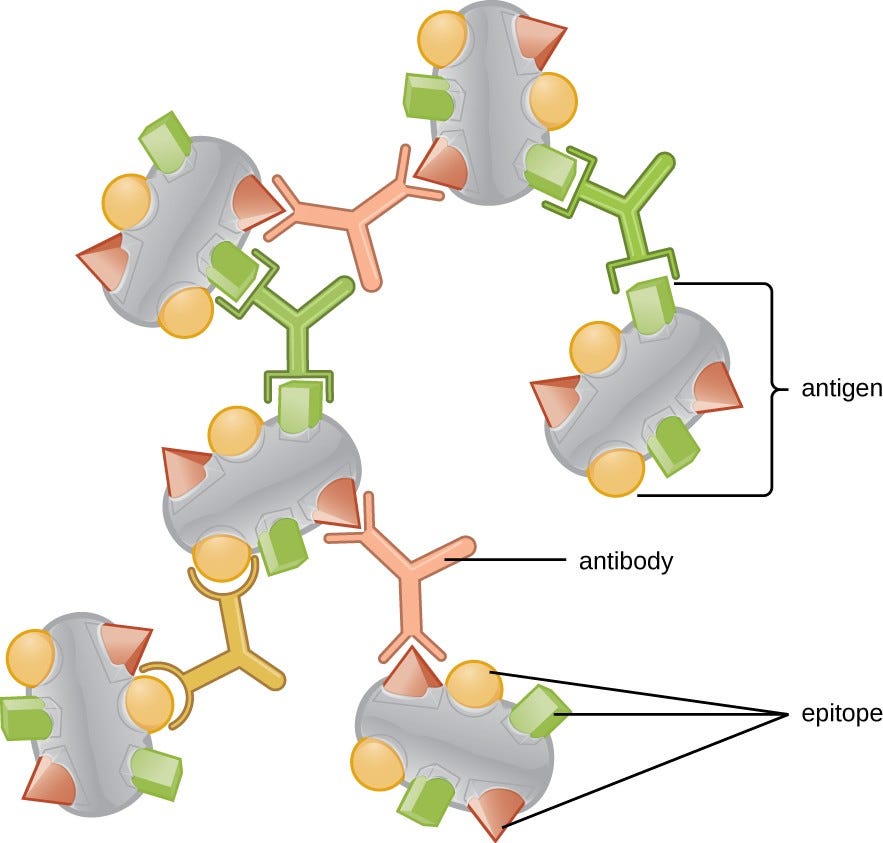
An immune complex, sometimes called an antigen-antibody complex is a structure that forms when antibodies adhere to antigens.
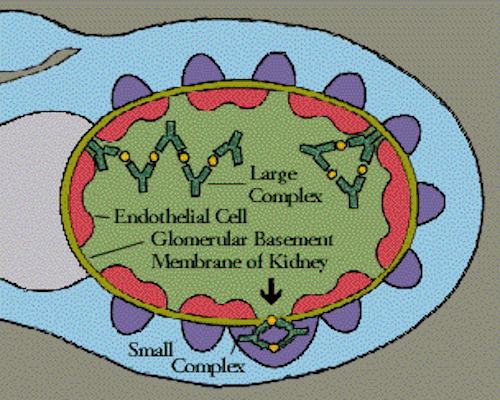
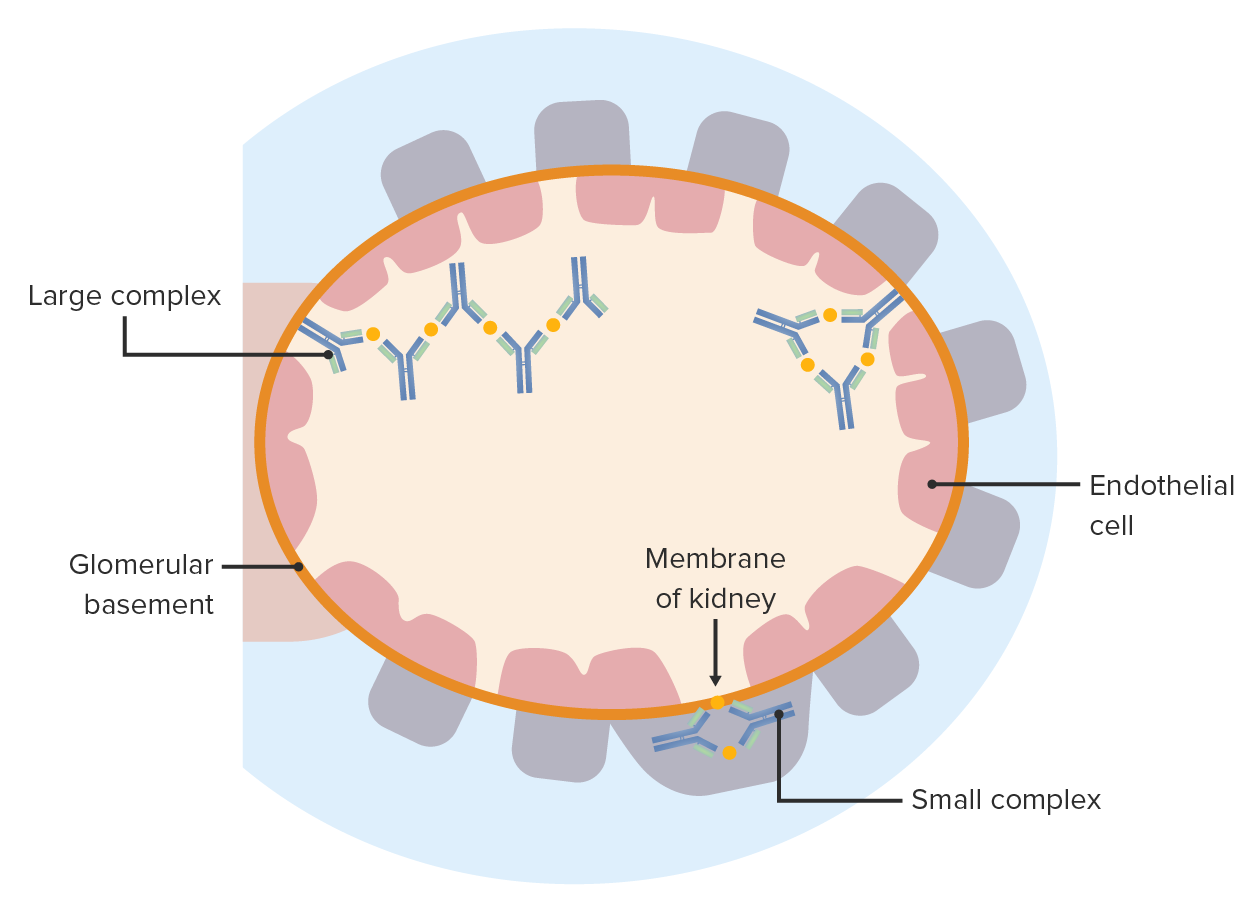
Immune complexes may themselves cause illness when they are deposited in organs.
Antibodies may bind to viruses without necessarily mediating their neutralization and/or removal. Such a binding may even be deleterious, as it may facilitate entry of viruses into cells – one example being the colonization of macrophages by HIV.
Pathophysiology and clinical manifestations of immune complex vasculitides
Immune complex vasculitides present inflammations of vessel walls associated with and mainly elicited by perivascular deposition of immunoglobulins, mostly in the form of immune complexes (ICs).
The deposition of immune complexes in the vascular wall is one major igniting factor of the local vasculitic reaction, mainly by activating polymorphonuclear leukocytes.
To produce a precipitin reaction, varying amounts of soluble antigen are added to a fixed amount of serum containing antibody.
In the zone of antibody excess, each molecule of antigen is bound extensively by antibody and cross-linked to other molecules of antigen. The average size of antibody-antigen complex is small; cross-linking between antigen molecules by antibody is rare.
In the zone of equivalence, the formation of precipitin complexes is optimal. Extensive lattices of antigen and antibody are formed by cross-linking.
At high concentrations of antigen, the average size of antibody-antigen complexes is once again small because few antibody molecules are available to cross-link antigen molecules together.
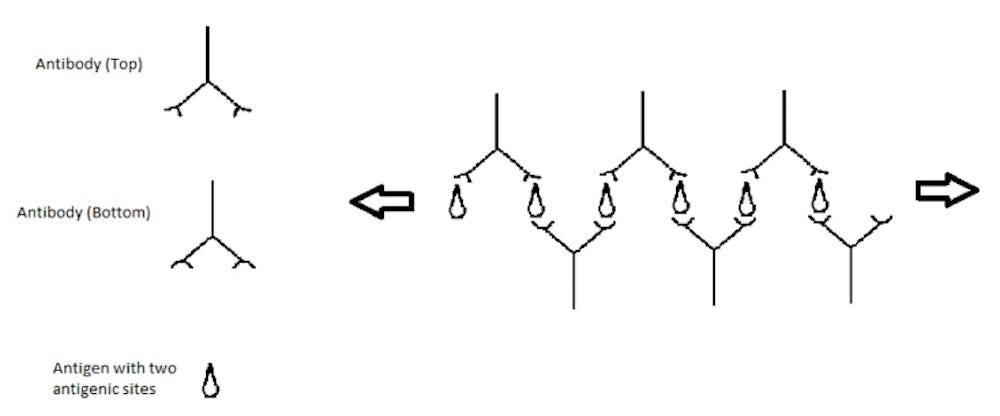
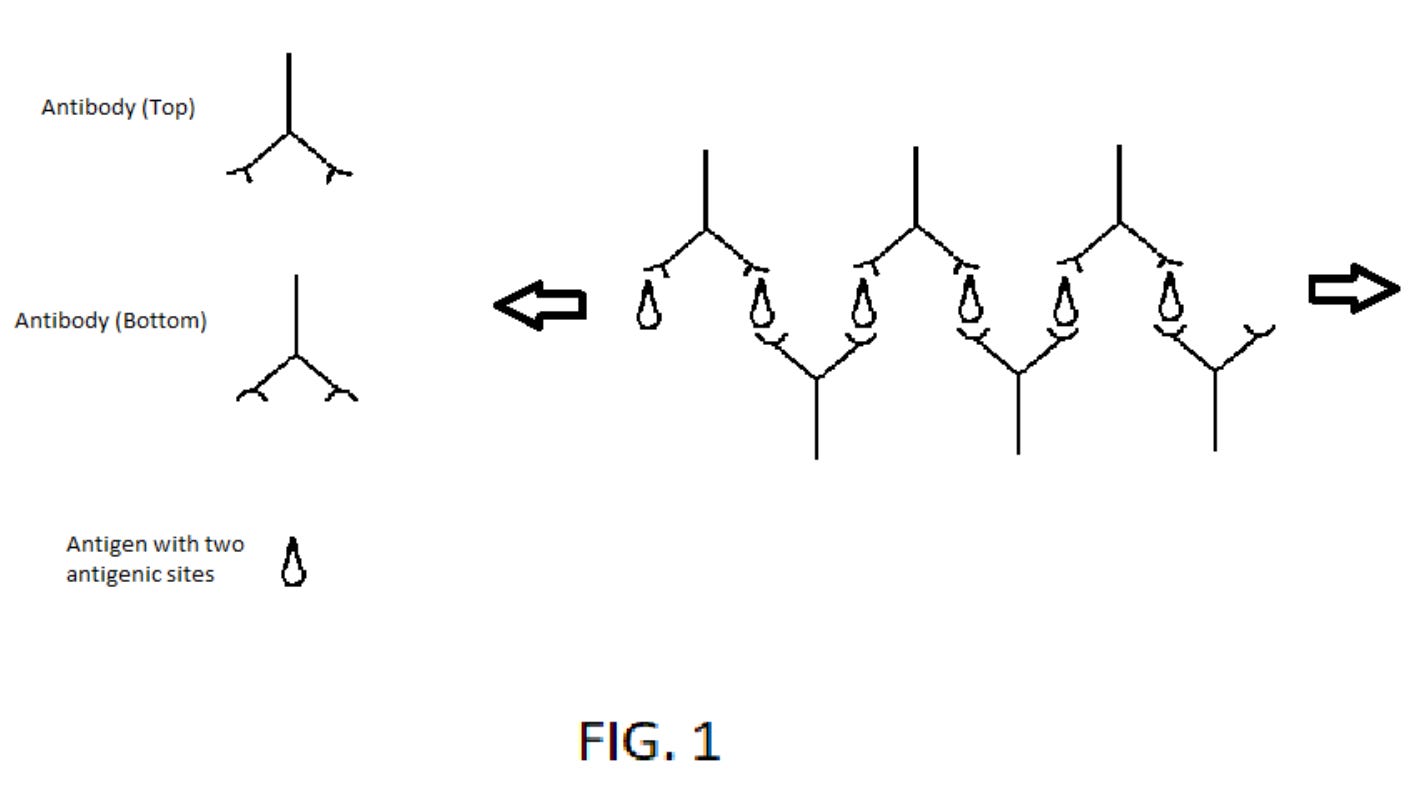
When a virus presents its surface antigen to B-lymphocytes, only the TOP of the antigen is presented for later antibody production. But, for a free antigens not attached to a virus particle, all sides of the antigen molecule can produce corresponding antibodies. It is impossible for a vaccine scientist to argue this point and say otherwise.
After the first vaccination to an X virus, a child will form antibodies to both the TOP and the BOTTOM of the free X antigen. Many more distinct antibodies may have formed, but we only need these two and the X antigen to produce strings of antibodies.
Following the second vaccine to X virus, we are absolutely certain of three facts.
1) antibodies to the top of the X antigen are present in the blood of this child for at least several months.
2) antibodies to the bottom of the X antigen are present in the blood for the same time period.
…
[If spike proteins are generated by transfected cells, escape the cells and then float freely in the body, the following could occur."]
Referring to FIG. 1, the booster vaccine results in X antigen in the blood. One arm of an IgG (Top) binds to the top of the X antigen (1). One arm of an IgG (Bottom) binds to the bottom of the same X antigen (1). The second arm of an IgG (Bottom) binds to another X antigen (2). One arm of a second IgG (Top) binds to the same X antigen (2). The second arm of the second IgG (Top) binds to a third X antigen (3). And the pattern can continue indefinitely, producing thick strands of antibody/antigen complexes. There can be many separate “strings” of alternating IgG (Top) and IgG (Bottom) antibodies. Can you see how this meshwork of strings is the basis for clots?
The bad news doesn’t stop for the vaccine industry. All IgG antibodies have an FC region. All platelets have moderate expression of FC receptors. These FC receptors activate platelets when an immune complex attaches to the platelet’s FC receptors. Activated platelets form clots in the blood. This meshwork of antibody strings is full of immune complexes that can each activate the platelets that are trapped within this meshwork. Activated platelets activate the coagulation cascade to add fibrin to the meshwork of antibody strings, platelets, and now fibrin.
Micro-clots in the capillary system of the brain can cause damage to the nervous tissue supplied by that particular capillary. It may cause an infarct small enough not to be easily detected by a CT scan or MRI. A clot in the capillaries of the heart can cause small infarcts in the myocardium.
This is NOT a scenario easily reproduced in a natural setting. A patient with a viral infection is unlikely to be infected again with the exact same virus within four months for many reasons. The chance of the patient developing natural antibodies to X virus, then being exposed to the X virus again, and being re-infected within five months is highly unusual. So, the clot issue is very unlikely with naturally occurring X viral infections (without vaccines) compared to the situation with the vaccinated.
Even IF a patient develops X viral infection and forms X antibodies and three months later, the patient is re-infected with the same strain of X virus, the chance of an immune complex causing clots via the platelet mechanism is extremely low in the natural setting. When the patient is exposed to the X virus the second time, free X antigen not connected to the X virus is unlikely to be found in the blood. The X antigen will most likely be attached to the X virus. That is technically an “immune complex”. However, the bonding of the IgG antibody to the X antigen that is still attached to the X virus is much stronger than the bonding of the FC region of the X antibody to the platelet FC receptor. Within the turbulent flow of blood, the X antibody can’t connect the X virus (at least 100 microns in diameter) to a platelet (at least 500 microns in diameter) with one IgG antibody in between the X virus particle and the platelet.
The kinetic force of moving plasma/blood components will rip apart the virus particle and the platelet, which are supposedly connected by an IgG antibody. So, in the natural setting of being exposed to X virus and being infected with the X virus twice within four months, that occurrence itself is improbable and very rare, and in the natural form, X antigen is attached to the X virus and highly unlikely to create an “immune complex” that can stay attached to a platelet’s FC receptor.
Also, it is highly UNLIKELY that the body will form antibodies to the bottom of the X antigen since the X antigen presents to the B-lymphocyte ATTACHED to the X virus and so the B-lymphocyte rarely will see the X antigen separate from the X virus. Furthermore, in a natural infection with an X virus, it is unusual for the B-lymphocyte to be exposed to the X antigen separately from the X virus, which means antibodies to the bottom (or portion of the X antigen that attaches to the virus particle) of the X antigen is unlikely ever to form. Unless there are two distinct antibodies that are formed to the same X antigen, but to distinct antigenic sites on the X antigen, the X antigen will not be able to act as the glue, connecting the distinct antibodies that form to the same X antigen, as illustrated in FIG. 1.
It should be absolutely clear that in the natural setting of being exposed to a natural virus, the situation described in FIG.1 is rare because 1) a surface antigen attached to a virus does not present the antigen’s attachment to the virus particle to the B-lymphocyte and 2) when the surface antigen is actually attached to the virus particle, it is too large to actually act as glue for distinct antibodies to the same very large antigen. The antigen size that is most effective to act as glue for distinct antibodies are antigens that are sufficiently small so that one arm of one antibody can bind to one area of the same antigen and the other arm of the same antibody is allowed to bind to a different molecule of the same antigen.
A hepatitis B infection is an exception in that HEB B Surface Antigen (HBsAg) is formed by infected cells in incredibly large numbers, much greater than the numbers of infectious virus particles that are produced. This is further discussed in a different part of this letter.
So, for a four-year-old child, the chances of antibodies forming chains is virtually non-existent, except for certain viral infections. But, a four-year-old child that has had all their vaccines over their four years of life, that child will have had at least 10 booster vaccines, each of which can create the strands of antibodies as described above.
In the vaccine setting, almost EVERY vaccine booster (that provides an inactivated toxin or a viral surface antigen only) within six months of the first vaccine can create “immune complexes” that can cause clots. With every vaccine booster, you expose the patient to a significant risk of increased clotting with all the downstream effects of blood vessel blockage in the respective organs. When the vaccine is comprised of a smaller antigen, smaller than an IgG antibody, strands of antibodies can form.
When a meshwork of antibody strands become tangled within a smaller blood vessel and platelets become trapped in this meshwork, then every FC region of every antibody within the strands can bind to receptors on the platelets and this activates platelets to initiate coagulation, fibrinogen is converted to fibrin, and you have a thrombus formed inside the lumen of the blood vessel. An antibody combined with its’ antigen is called an “immune complex.” Within these strands of antibodies, held together by the antigen glue, almost every antibody is in the form of an “immune complex,” which is very well known to be able to activate platelets.
And all these vaccines have been mandated for children for decades. Most vaccinated children before the age of 4 have at least a dozen times when they have extended strands of antibodies in their blood , with all the risks of clotting from those immune complexes. Let’s say those micro-clots occur in a capillary to the amygdala of a developing two-year-old brain. Then those micro-infarcts could result in ongoing permanent anger issues for the child. In other areas of the developing child’s brain, micro-infarcts can result in behavioral and mental changes. I can give a million examples.
What I show is that each and every antibody formed in response to an antigen will be almost guaranteed to bind to that same antigen that is given in the booster vaccine. But the chance of that same antibody binding to that same antigen on a real virus is probably less than one in a million. In essence, what the vaccine industry considers the main beneficial effect occurs so rarely, that if a side effect occurred at this incredibly tiny rate, it would not even be listed in their very long list of side effects. In conclusion, the effect of antibody strand formation with a booster vaccine… is almost guaranteed and the formation of a clot is almost guaranteed.
This meshwork formation of antibodies after a booster vaccine isn’t a side effect. It is by far the MAIN EFFECT. So, immediately halt the sales of all vaccines until you wrap your collective heads around this massive issue. That is the only rational response.
I show such a clear connection between vaccines, clots, and autism, it’s time for the vaccine scientists to acknowledge that their gig is up. Their science is sloppy, and they engage in extreme cult-like behavior. The HEP B vaccine for infants is the modern-day equivalent of human-child sacrifice. There isn’t a pediatrician on earth who can explain how COVID antibodies can efficiently cross the lung barrier to enter the area of the lung infected by the COVID virus. There is only risk when you can’t show benefit to your intervention. And if you point a gun (with 3000 empty chambers and one bullet) at a child and pull the trigger, you are ONLY exposing the child to risk, and you are a baby killer. I highly doubt that vaccine scientists have looked into any of this. They are so busy telling the parents of children who had severe side effects shortly after their vaccines that it was NOT the vaccine that they were never going to open their minds and see the big picture.
If just one retail pharmacy chain does the right thing and openly questions the vaccine industry in response to this letter, the others will be forced to follow suit, and the world will realize the sheer stupidity of mandating childhood vaccines and children forever can be spared this modern day form of human child sacrifice and torture.
In the history of medicine, there will never be another paradigm this established that is destroyed with only ONE DIAGRAM (FIG. 1); this ONE PIECE will cause the paradigm shift that is realizing that antibodies are not useful in our fight against viruses. Be on the right side of history; protecting our children.
Signed,
Joseph Y. Lee, MD
SOURCE:
Covid Vaccine Irrefutably Linked To Clot Formation
As additional information is gathered, I will add it below...
Immune complexes may themselves cause disease when they are deposited in organs, e.g. in certain forms of vasculitis.
Type III hypersensitivity occurs when there is little antibody and an excess of antigen, leading to small immune complexes being formed that do not fix complement and are not cleared from the circulation. It is characterized by solvent antigens that are not bound to cell surfaces (which is the case in type II hypersensitivity). When these antigens bind antibodies, immune complexes of different sizes form. Large complexes can be cleared by macrophages but macrophages have difficulty in the disposal of small immune complexes. These immune complexes insert themselves into small blood vessels, joints, and glomeruli, causing symptoms. Unlike the free variant, small immune complex bound to sites of deposition (like blood vessel walls) are far more capable of interacting with complement. These medium-sized complexes, formed in the slight excess of antigen, are viewed as being highly pathogenic.
Such depositions in tissues often induce an inflammatory response, and can cause damage wherever they precipitate. The cause of damage is as a result of the action of cleaved complement anaphylotoxins C3a and C5a, which, respectively, mediate the induction of granule release from mast cells (from which histamine can cause urticaria), and recruitment of inflammatory cells into the tissue (mainly those with lysosomal action, leading to tissue damage through frustrated phagocytosis by polymorphonuclear neutrophils and macrophages).
Conclusions: Our findings uncovered a novel function of SARS-CoV-2 on platelet activation via binding of Spike to ACE2. SARS-CoV-2-induced platelet activation may participate in thrombus formation and inflammatory responses in COVID-19 patients.
On the Role of Platelet-Generated Amyloid Beta Peptides in Certain Amyloidosis Health Complications
Adverse Events Following Immunization With mRNA and Viral Vector Vaccines in Individuals With Previous Severe Acute Respiratory Syndrome Coronavirus 2 Infection From the Canadian National Vaccine Safety Network
The old system is crumbling, and we must build its replacement quickly.
If you are fed up with the government, hospital, medical, pharmaceutical, media, industrial complex and would like to help build a holistic alternative to the WHO, then feel free to contact me directly anytime.
Why was it so desperately important that Everyone be jabbed? I mean college tuition, lottery tickets, weed, burgers and fries, dates with escorts, etc? Politicians going on TV acting like cheesy furniture and appliance salesman selling the jabs. The media entertainment industry Bullying and browbeating the people to get jabbed.
Surely all of them didn’t Believe that there was a new bug that could spread around and kill millions. If they did they wouldn’t have done all the selling of the jabs in such silly ways, schlocky grade school ways.
So why? I ask for 3 years now. Someone handed the jab script to the world politicians. All of them. And only a few in third world countries saw through it. And died suddenly.
Will we who insist on Answers be died suddenlied? If we say that Jan 6 shooting was badly acted theater. If we say 9/11 pre planned demolitions were done at the behest of the same folks who wrote the Covid script.
This was a mind blower! He made absolute sense. I've become more aware of how nothing is as it seems and the fact that NOBODY will even discuss it and is actually running is very suspicious to me!






























Why was it so desperately important that Everyone be jabbed? I mean college tuition, lottery tickets, weed, burgers and fries, dates with escorts, etc? Politicians going on TV acting like cheesy furniture and appliance salesman selling the jabs. The media entertainment industry Bullying and browbeating the people to get jabbed.
Surely all of them didn’t Believe that there was a new bug that could spread around and kill millions. If they did they wouldn’t have done all the selling of the jabs in such silly ways, schlocky grade school ways.
So why? I ask for 3 years now. Someone handed the jab script to the world politicians. All of them. And only a few in third world countries saw through it. And died suddenly.
Will we who insist on Answers be died suddenlied? If we say that Jan 6 shooting was badly acted theater. If we say 9/11 pre planned demolitions were done at the behest of the same folks who wrote the Covid script.
I can’t wake up even one NPC.
This was a mind blower! He made absolute sense. I've become more aware of how nothing is as it seems and the fact that NOBODY will even discuss it and is actually running is very suspicious to me!